
I have been critical of arguments used in Independent Medical Examiner (IME) reports to justify opinions that a work injury (or an activity at work) is no longer the “cause” of an ongoing disabling condition. My criticism is based on the faulty logic of those opinions under our current legal system, not because I have no sympathy or concern for the employer found to be liable when those arguments fail.
One of the most common opinions expressed in defendant IME reports is that the effects of a work injury have ceased and that any ongoing symptoms are due to an underlying degenerative condition.
The spurious argument
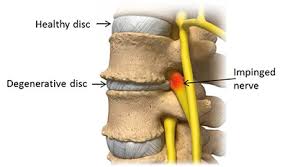
There is an underlying asymptomatic degenerative disease, usually evident as imaging changes. No argument with that! Although there is an acceptance by the IME that an injury, event or a work activity triggered the claimed condition, the opinion is, that despite continuing symptoms, the effects of the injury or work activity have ceased (or will cease at some future time). Therefore any continuing symptoms (and associated disability, work incapacity or need for treatment) are solely due to the underlying condition which is unrelated to work. It is argued that the effects of the claimed injury can only continue for a finite period of time, often on the basis that the inciting injury was minor.
It is the latter arguments that fail the test of logic. I know of no evidence to support the idea that the duration of symptoms following an injury in a compensation system can be accurately predicted, nor evidence about the likely timing of onset of symptoms from an asymptomatic degenerative disorder. Certainly the IME’s who use these arguments do not present any evidence in support. There are however well accepted mechanisms for persistent pain that can explain chronicity of symptoms irrespective of the severity of any initial tissue damage.
What is fair?
I do have sympathy for the insurer or employer where a claim is made for a seemingly minor incident at work on a background of gross reportedly asymptomatic degenerative disease and the claimant develops long-term incapacity. The employer has to cover treatment, including expensive surgical procedures and income support costs and perhaps a significant payment for permanent impairment.
From a medical perspective, the most significant cause of the claimed condition might well be the worker’s genetic makeup and their life-time of wear and tear activity. The ‘straw’ that breaks the proverbial ‘camel’s back’ (or in the situation being discussed here, the ‘insurer’s purse’) is often a fairly inconsequential injury or event at work, or even onset of symptoms in the course of normal work activity.
Workers compensation liability determination however works within a legal framework. In most jurisdictions, an ‘injury’ arising in the course of employment is all that is required for liability to be placed on the employer for treatment, lost income and permanent impairment. It doesn’t matter much how significant the injury was, or whether there were predisposing factors, if the person was previously asymptomatic, there is a good chance that the employer will be found liable.
Furthermore there is the principle of benevolent interpretation, especially when it comes to impairment assessment. For example, in the current version of the Tasmanian WorkCover Guides to the Assessment of Impairment, the following appears:
‘If there is objective evidence of a pre-existing symptomatic permanent impairment in the same region at the time of the work-related injury, then its value should be calculated and subtracted from the current whole person impairment value. If there is no objective evidence of pre-existing symptomatic permanent impairment, then its possible presence should be ignored.’
The reference to ‘symptomatic’ in the final sentence above is true benevolence, because for a pre-existing condition to be considered significant and taken out of consideration it has to symptomatic, in addition to the requirement for objective evidence of its existence.
Presuming that the worker is telling the truth (and that is not always correct) there are adequate medical explanations for persistent pain following injury i.e. the mechanisms of neural sensitisation and the influence of psychological factors on those processes. It is perhaps wishful thinking that a doctor can arbitrarily state that the effects of the injury have ceased and that the persistent pain and disability has somehow reverted to being due to the underlying condition even if the process had previously been asymptomatic. The ‘but for’ test comes into play from a legal perspective i.e. ‘but for’ the injury/event/work activity, is it likely that the worker would have the current symptomatic condition?
In reality, in most cases, the only logical answer is that without the work injury/event/work activity the worker would not have the symptomatic condition and therefore the employer is legally liable. It is a separate question as to whether that is fair. As our workforce ages with the expectation from our politicians that we will all work longer and longer these issues will become more and more common.
In my opinion it is usually a nonsense when an IME assessor uses the argument that the effects of a precipitating event has passed and that a previously asymptomatic condition has now taken over as the cause. It doesn’t make medical sense, nor is it ‘common sense’.
The real question?
What is needed to avoid employers becoming unfairly liable for degenerative disease resulting from genetic predisposition and a lifetime of wear and tear?
While it will be a difficult task to change currently well-accepted definitions of causation established by statute and common law, such changes are essential to ensure the burden of occupational injury and disease is fairly borne by employers. Maybe any change will open up a whole new opportunity for legal argument! I certainly hope not.
There are many conditions where work is the cause, but no claim is lodged, or claims are legislatively excluded, particularly burgeoning workplace psychological ill-health issues. If the system is to fairly deal with these conditions, which it does not at present, measures need to taken to reduce the burden on employers from unfair liability for degenerative musculoskeletal disorders.
The answer
A change to the legal definition of injury such that medically recognised contributing factors can be taken into account in determining liability, even for previously asymptomatic conditions.

Peter, I well remember encountering such arguments in the reports of my colleagues who examined my patients at the request of third party insurers. My immediate reaction was – how on earth do they know such things? Gazing into their crystal balls, perhaps? But I cannot see how changing the legal definition of injury would alter this situation in compensation systems where one doctor’s opinion is valued as being equal to that of another. Is not the main object of an IME assessment to help third party payers convert medically-assessed percentage whole body impairment into hard cash? If so, this is always going to be a scientifically unsatisfactory exercise and open to abuse.
Agree with John.
Would like both your opinion on the following-
1. What about the case where, in the face of no objective evidence of any degenerative condition ie not reported in imaging studies at the time of the injury, but 15 years after the injury an assessor viewing the original images states there was a degenerative condition and then deducts a large percentage due to his own reading of 15 year old images?
2. What about the case where the person is injured and liability accepted and treatment ensues but there is the normal degeneration after the injury when there is no pre-existing condition. There are assessors then deducting for post injury degenerative change. Is this a “but for”case and are the assessors correct in their interpretation?
3. I would guess you would have to be very familiar with the WorkCover /AMA 5 Guides for ROM testing. The guides give a very clear instruction for performing say, for example, shoulder ROM.
-The test methodology would have to have been designed using scientific methodology in a research situation in order to establish the applicable score charts. Would you agree?
-It seems to me the guides make it clear the methodology must be adhered to in order that the score charts give valid results. Would that be a correct interpretation?
-The validity of the result is also dependent on repetition of each test in the manner described to enable an average to eliminate bias and to determine consistency. Would you agree?
-Now the point becomes one of what happens if the IME is carrying out the ROM testing in a manner other than the AMA 5 describes such as internal rotation behind the back measured to the vertebral height. There seems no means of scoring this with the score charts applicable to the rotation tests as described in the AMA 5 but some assessors are providing scores for this method without undertaking the method set out in the AMA 5. Is this inconsistent with the guides as set out and consistent with the intent of what is to be measured?
-Another point in relation to shoulder testing is the matter of a person who cannot achieve the starting point for the rotation tests. The test methodology for the rotation tests is clear and in my opinion if the applicant can’t reach to starting point then the charts cannot technically be applied and the injured worker would have to be considered fully impaired in the Range of Motion the test is applicable to. How would you see this?
-Some assessors are testing shoulder rotation at any degree of abduction, for example, an injured worker who can only abduct their shoulder to 20 degrees who then carries out the rotations from this position is being scored from the AMA 5 rotation charts in the same manner as someone who is able to abduct to 90 degrees to carry out the rotations in the manner described as per the guides. There must be some scientific, biomechanical basis behind the design of the methodology as there are different forces and mechanical loads on the muscles when they are used in different positions. I can see this and I would expect a high school student knows about fulcrum and load or a physicist or an engineer or a shoulder surgeon could explain it better than me. The scores give the perception the two injured workers have the same impairment when one is in fact much more impaired. As a teacher I am an expert in test methodology and I know if you vary the method you invalidate the test and you don’t know what you are measuring. What is your opinion on this inconsistency?
4. It is clearly stated in the AMA 5, the shoulder ROM tests should be carried out from the neutral starting point which is the generally accepted anatomical position with the applicant standing erect, the hands by the sides and palms facing anteriorly. There are cases where this is being disputed and it is stated just because the neutral starting position is defined the assessor is not expected to carry out the tests with the palms forward, and cases where the assessor carried out the shoulder ROM tests with the injured worker lying on their stomach. The judge in that case stated this was a valid method of testing the shoulder ROM testing even though the argument was put that physics would show this method would not produce valid results according to the score charts. The expert witness for the injured worker explained the need to comply with the AMA 5 but no one pointed out that the neutral starting position was the erect position and the judge stated the AMA 5 made no specific reference to this so the injured worker was allocated zero shoulder impairment and lost the case even though it was agreed the ROM tests were carried out lying down. What is your take on this type of inconsistency? Not logical to me!!
Would appreciate some discussion on the validity of the guides if it is being accepted some assessors are basically using what ever methods they want.
Good to hear a range of opinions on your website.
In this context the law requires certainty, which the US AMA Guides cannot deliver (as we all live in an uncertain world). The reliability of the Guides was discussed by Forst, Friedman and Chukwu (2010). They suggested that a research agenda should include investigations of reliability and construct validity for different body sites and organ systems along the entire rating scale and among different categories of raters. I am not aware that such research has ever been published. Peter may correct me on this.
Reference: Forst et al. Reliability of the AMA Guides to the Evaluation of Permanent Impairment. J Occup Environ Med 2010; 52 (12): 1201-3.
Thanks Justice Seeker
The concept of impairment assessment is entirely artificial and has arisen out of a need to put a percentage on the effects of injuries for compensation purposes. What is actually being measured by AMA4 or AMA5 methodology is not clear, but the percentages obtained should be reproducible between examiners if done according to prescribed methods.
In my experience many assessors can’t be bothered to follow the prescribed methodology and just use their standard clinical approach. This is particularly so for hand and digital ROM assessment – I presume they can’t be bothered to separately measure each joint’s ROM.
In answer to your queries:
1) The IME assessor sounds a bit dodgy to me
2) I don’t think to deduct degeneration occurring after the injury is correct, the most likely scenario is that the injury caused or significantly contributed to the degeneration
3) & 4)The prescribed methodology is clear and should be reproducible between examiners, but is not necessarily valid as the whole concept is artificial.
From your description of how the IME approached the ROM assessment it seems clear that he/she doesn’t understand the prescribed methodology for shoulder ROM assessment. The methodology for internal and external rotation testing is with the patient standing erect and the shoulder abducted to the horizontal position, not the standard clinical method how far the patient’s thumb can reach up the spine. The assessment should be shown to be invalid if tested in court. Your point about the neutral starting point to be able to test for internal and external rotation is valid – it does make it difficult unless there is abduction to 90 degrees. The correct test position for all shoulder range testing is with the patient standing in the so called anatomical position, but I’d have to look at AMA5 to see if there is a definite reference to confirm that. I don’t have my copy of AMA5 with me at the moment, but the diagrams in AMA4 certainly confirm the testing is done with the patient standing (including testing internal and external rotation) and my recollection is that AMA5 is the same. In Tasmania our ratings are still done using AMA4!
Does this help?
Peter Sharman
Yes, it certainly does!
The most concerning thing is that this all relevant to some Approved Medical Specialists working directly for the Workers Compensation Commission in NSW. We are raising the matter of the lack of consistency in the application of the NSW WorkCover Permanent Impairment Guides that rely on the AMA 5. They state ROM testing MUST be carried out using the tables, graphs and methodology as per the AMA 5. The measurement methodology chapter (don’t recall chpt no. off hand) definitely describes repeating the ROM tests three to six times to determine the average etc for a consistent result. It is also states a goniometer should be used but this does not seem to be a regular occurrence as far as we know, however some AMS/IMEs are stating in reports that a goniometer has been used at times when this is not the experience of injured workers so another concern for injured workers is that “guessing” is the main method of measuring. In NSW It is very hard for an injured worker to challenge an AMS as there is a presumption of correctness in aspects of their findings ie, Under section 326(1) of the Workplace Injury Management and Workers Compensation Act 1998, the following matters in assessments certified by an Approved Medical Specialist (AMS) are conclusively presumed to be correct in proceedings before the Commission:
(a) The degree of permanent impairment of the worker as a result of an injury;
(b) Whether any proportion of permanent impairment is due to any previous injury or pre-existing condition or abnormality;
(c) The nature and extent of loss of hearing suffered by a worker;
(d) Whether impairment is permanent; and
(e) Whether the degree of impairment is fully ascertainable.
The legislation only allows Appeal on a limited basis and it seems to have devolved into the case where the AMS’s status is being looked at as the basis of him being correct regardless of what he/she does and this is very hard for an injured worker to deal with. Many injured workers would like to see an inquiry into this.
In regard to the AMA 5, we did examine a copy and found it much the same as the AMA 4 except one of the score shoulder ROM charts in the AMA 4 seems to be upside down compared to the AMA 5.
Another matter that is of concern is the fact some IMEs and AMSs are recording that they are repeating the ROM tests saying they have carried them out “at least three times” or “several times” when they are not actually repeating the tests at all to enable them to get an average, just relying on the one set of tests apparently so they can get you out the door ASAP. Also of concern is the fact some assessors claim all movements are active knowing they are either directing the worker to self assist or are passively moving the limb themselves. The NSW guides only distinguish between passive and active motion and in some cases the assessor is directing the injured worker to self assist and it is interpreted as though this is passive motion, not to be scored, while other cases say this is said to be active and is being scored, thus another inconsistency. Are you having such problems in TAS? Injured workers complain of this type of thing but they often fail at Appeal because the legislation states the AMS is “conclusively presumed to be correct” so Appeal Panels are interpreting this as “the AMS can’t be challenged” so unless there is other evidence in the Medical Assessment Certificate itself that may indicate the AMS has made an error the injured worker virtually has no voice. This is all really concerning as the AMSs in NSW are also those on the Appeal Panels so they are judging each others errors. A conflict of interest don’t you think? The new 2012 legislation now only gives an injured worker one go at a WPI % so if they strike an IME or AMS who is not applying the test methodology consistently they are basically up the proverbial “s–t creek”! The percentage of permanent impairment is being used to determine the level of all benefits in NSW with no account of pain and suffering allowed at all. People who are disabled due to high pain levels but who may only be assessed at 10% WPI or under are losing all support in an arbitrary time frame that is now applied according WPI. The system really lacks understanding of the multitudinous aspects of injury and the impact on someone’s ability to work. Is this the case in TAS?
It is good to see there are doctors like you who are doing the right thing and who do know what is really going on as it is certainly a minefield for the injured.
Thanks for your response, it verifies for us we are right in our understandings. We (my husband and I) are members of the NSW, IWSN and we are trying to reveal the facts about what goes on inside the examination room. Many injured workers are now beginning to want video recording of assessment but this has a long way to go as there are other legal implications, however there is also a thought that history taken in the assessment room should be photo copied and provided to the worker as they leave the examination for verification as well as use of proforma recording sheets that show the scores as they are taken, where the worker can sign off a check list on what or how many times the tests were done, that a goniometer was used, that only active motion was scored and if the person could not complete the tests in the correct manner this should be stated rather than just a made up score on a page. In both my case and my husband’s case we were able to obtain the handwritten notes that showed what the assessor reported was opposite of what they recorded in their notes in certain aspects. Of course this is a simplified view but there needs to be some movement toward greater oversight as it has just become too easy for some assessors to be complacent or even to be under the influence of one party or another to the extent it has created the possibility of financial gain influencing their portrayal of results. In NSW the AMSs working for the WCC also work as IMEs for either party providing another layer of conflict of interest.
Most injured workers only want their medical treatment and some means of maintaining the ability to feed their families and to keep a roof over their heads.
Interested to hear your views and solutions for such things.
Thanks again for being forthright and honest.
Hello Doctor, very much appreciate this blog. It will be twelve years in May since my car accident coming home from work, I have been through a very hard time with insurance IME’s through this drawn out period of just wanting to get fixed, I damaged my lumbar, both knees, was basically squashed when my head and back (thorax) kept hitting the car ceiling, repeatedly hit into my sister’s head and shoulder area during the MVA but the worst part is the neck, 3 or the discs damaged in the cervical region have shrunk a bit but the fourth worst disk is 5/6 with the disk squashed and worsened, worse in the annular area and development of stenosis both sides (foramina) leaning on the nerves very plain in the MRI. Well the insurer was upset that it had worsened so sent me 500 kms for an appointment with one of their neurologists. When I got there I was told the appointment was changed 8 weeks previously to another neurologist in Martin Place with noone telling me prior to this. I could not stop crying as I was already nervous I have had some pretty unhelpful and nasty insurance doctors in the past and it has a terrible effect on the nerves too. The insurer said they knew nothing of the change of doctors so who did then? I was sent to a very old gent I had my new MRI and xrays, he said he didnt need to see them he had all he needed on his desk. On his desk were a stack of psychological reports. He didnt care about the MRI, he decided to state on his report that I wasnt fit for work due to a “mood disorder” triggered by the accident but he said the cause was child abuse I suffered when a small child. It is true that I was abused, I however did attend a lot of counseling in my twenties to put as much behind me as possible. I was 39 when I was hurt, was not in any pain whatsoever previous to the MVA, I was fit, I went to the gym regularly and my life was going well, I worked weekends helping the disabled and during the week starting a business in airbrushing. Due to the injuries and pain and numbness particularly the radiculopathy, my dreams of that business are over. I had the solicitors send me my massive file, after my solicitor was disbarred a large law firm kept my file with no action for years. So one of the insurers old forensic psychiatrists put a little note in to the insurer that “she probably did the injuries at the gym” this was a note between them I was not meant to see.
This is Australia and I have still got to fight for an operation after nearly 12 years because of this system. They make me cry.
Kerrie, I know it will not help you but I would like to apologise for the despicable behaviour of those of my medical colleagues who examined you and wrote such ridiculous reports. They can have only added to your distress!
Thank you John it has been a nightmare and as I only want the truth so I can know how to deal with my injuries and get the help any Australian would expect I find it horrifying that doctors are lying to make money, there are incredible decent doctors all around the world and these insurance quacks are plain out commiting purgery when they side with insurers against genuine cases, how does an accident victim have to still be waiting for and operation for twelve years and the government backs these people. Mr O’Farrels callous “legislations” have causes family breakdowns, homelessness and suicides yet the media focus on the rare cases of fraud while the insurers are consistantly committing fraud. so how does one fight back while ill? I would like to thank both yourself and Peter for adding some sanity to this wicked greedy farce.
P.S. since when are neurologists becoming psychiatrists,i would have thought a nerve conduction study more as to what he should have offered
There is lot to be desired in the standards of some IME assessors
Too true and yet noone investigates them for the malicious damage they cause, Peter, you and John are legends in my book:)
Kerrie, I once witnessed a noisy demonstration outside the WA Parliament. The unions were protesting about changes to the Workers’ Compensation legislation that appeared to them as draconian. Some members of the Injured Persons Action and Support Association (IPASA) wore face masks and carried banners on which were displayed the names of each of the most notorious “insurance doctors” in Perth. The demonstration was covered by the media. Guess what happened? Nothing changed and the “named and shamed” medicos continued on with their work as if nothing had happened. It brought home to me the extent to which injured workers in our society had been stigmatised. And a profession that had once safeguarded its high standards of ethics and care had let them down rather badly.
Yes, we live in a society where commercial interests are considered above all else and human rights are slyly snuck away with impetus.I am beginning to think only a royal commission and a class action are about all we have left to help us, there is no duty of care applied and our constitutional rights are being squashed. An old solicitor a few years ago looked at my file and said I had reports from at least 5 of the worst “i”me’s that insurers use to consistantly disagree with better qualified doctors, just too much corruption! Our ancestors who fought for our rights and for fair help for the injured would be turning in their graves.
and what percentage did I get from the insurance doctors against the percentage given by a more honest doctor? Get this…0% yet as they know I am permanently injured I currently get the higher rate of pay for now, until they stop it and i need just the pension which would not cover the rent so this is terrifying I have a child to raise.
and I have never had a ROM test with averages always only done once without use of any goniometer