This article follows on from my recent article about complexity in workers compensation systems that refers to the concept of ‘complex case management’ by experienced medical practitioners.
Reducing Complexity for Injured Workers
The AMA in Tasmania, through its workers compensation reform committee has put forward a proposal that builds on the concept of defining roles for doctors within our workers compensation systems with a proposed role of ‘Complex Medical Case Manager’.
Definition of this role, along with the development of processes to identify poor prognosis cases early, is a key plank in the reforms proposed by the AMA to improve health outcomes for injured workers.
I do have a vested interest in the concept of ‘complex case management’. In effect, this is what I do when an injured worker is referred to my practice by their general practitioner for ongoing management of their injury. A proactive role by a doctor co-ordinating medical management with a strong focus on recovery and rehabilitation can overcome some of the barriers to recovery inherent in our compensation systems by reducing complexity for the injured worker.
Managing a complex case takes interest, motivation, knowledge of processes and resources and experience along with a significant time commitment if it to be done well. It is important to achieve the right balance between promoting self-management by the worker while providing support and understanding. This is the ‘art’ of ‘complex case management’.
Sometimes taking on this role requires a willingness to undertake activities not usually undertaken by a doctor e.g. participating in meetings and conferences in a variety of locations and formats, visiting workplaces and talking to key people in the worker’s work and home life. The role requires skills in communication, co-ordination of the diverse group of practitioners involved in treatment, development of a consensus treatment plan and communicating that plan clearly to both the worker and the funding organisation.
A proactive doctor advocating a rational and co-ordinated management plan is sometimes welcomed by the insurer and employer, but at other times a co-ordinated approach by the treatment team is seen as a threat to control of the claim by the insurer or claims agent. There can be a fine line between acting as an advocate for an appropriate medical treatment and rehabilitation programme and becoming enmeshed in legal issues.
In my own practice to allow sufficient time to undertake this role, I set aside each Thursday free of clinic appointments to have the time to consider proactive case management, make telephone or email contact and prepare formal written communications with various key people involved. This cannot be done effectively while consulting. Managing a complex case cannot be done effectively at review consultations, even with relatively frequent appointments. Rarely these days can you contact another health professional, rehabilitation provider or insurance claims officer with a single telephone call. My day free of clinic appointments ensures I have the time to put together co-ordinated plans and communicate those plans to the relevant parties and my accessibility for returned telephone calls. ‘Telephone Tag’ is usually the name of the ‘game’, although email, fax and text communication plays a part too.
To me, detail is important in managing a case. Some might call it obsessional behaviour. The extra effort in making a telephone call to the worker or sorting out an apparent discrepancy between treater opinions can mean the difference between trust and distrust by the worker with their management programme, changing the focus from progress to stagnation.
I have kept records of the actual amount of time spent on managing complex cases that illustrate how a doctor’s time is spent in a proactive co-ordination role on complex cases.
I recently analysed my time spent on 5 complex cases over the last year or two. These include two cases managed by self-insurers, a case managed by a private insurer, a case managed by the Tasmanian State Service Compensation Scheme and one Comcare case. Each person was referred by their general practitioner for ongoing management of their work-related injury at my practice.
The time spent on these cases totalled 166 hours with 78 hours (i.e. less than 50%) of that time spent in face to face consultations with the worker and/or meetings with the rehabilitation providers assigned to the case.
The balance of time (88 hours in total) was spent as follows:
16% Telephone discussions with patient
15% Telephone discussions and email communication with other key people
7% Correspondence to other treaters
6% Correspondence & formal reports to non-treaters
4% Workplace visits
4% Other meetings
In another complex case not included in the analysis above there was a need to visit a dysfunctional workplace within a secure work environment where security arrangements meant multiple contacts with workplace and rehabilitation personnel to be able to gain first hand knowledge critical to understanding the dynamics affecting recovery. In this case there has been the need to interact with a rehabilitation provider, mediator, injury management co-ordinator and no less than 4 workplace people in addition to the usual number of treating health professionals including general practitioner, physiotherapist, psychologist and other medical specialists. In this case less than 25% of my time on this case has been in face to face consultations with the worker.
Are Doctors Pulling Back?
Complexity of compensation systems affects doctors too. A recently published study sheds some light on the phenomenon of increasing reluctance by doctors to get involved in treating patients within compensation systems. More and more doctors are being put off by the complexity of dealing with workers compensation as discussed in the following article. Surveys have shown that as many as 50% of general practitioners are now reluctant to get involved in the management of patients within complex compensation systems. In addition, some specialists simply refuse to see workers compensation cases.
Relevant Legislative Provisions
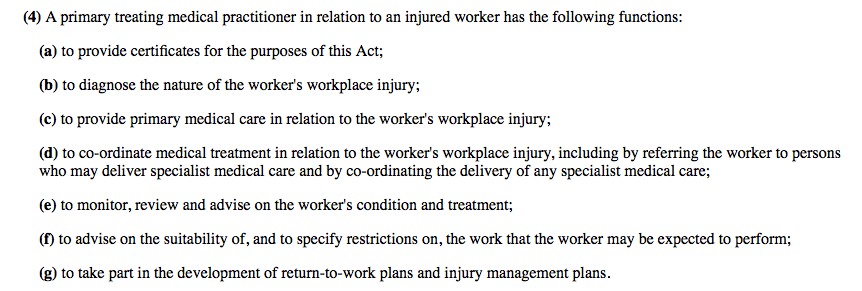
There are already some legislative provisions about the role of doctors in managing work-related injury. For example, Tasmanian workers compensation legislation sets out the role of the Primary Treating Medical Practitioner (PTMP) as follows:
The key item relevant to this topic is (d) above – the role of co-ordinator of medical treatment, usually undertaken by the worker’s general practitioner. The impact of this legislative requirement is difficult to determine, but I believe it is very useful for this to be set out as a guide to an important role in a compensation system.
Solutions
A solution to these problems involves reducing complexity for injured workers and their doctors to improve health outcomes and overcome the problems associated with doctors withdrawing provision of services within compensation systems.
An agreed ‘Best Practice’ approach to managing work related injury between the various stakeholders is the key. Mechanisms to facilitate streaming of injured workers into different management pathways according to their injury and prognosis should be developed. This approach would encourage early assessment and intervention to address risk factors for a poor prognosis, especially recognised psychosocial issues, and provision of medical and rehabilitation resources commensurate with the needs of each individual case.
General practitioners have a fundamentally important role in such early intervention. There needs to be a mechanism to provide education and support for doctors who want to be involved in managing patients in compensation systems, in addition to mechanisms for doctors to ethically make alternative care arrangements in circumstances where they do not have the time, knowledge, experience or interest to provide necessary care.
WorkCover Tasmania is trialling a
Medical Mentoring & Advisory Service (MAMS), provided by experienced general practitioners to guide doctors in the management of their work-injured patients. It will be interesting to assess the impact of this support initiative for general practitioners.
There should also be agreed processes to assist doctors to identify cases of work-related injury where additional resources are likely to be required that might be beyond the scope of the average time-poor general practitioner. This involves the development of screening tools to identify poor-prognosis cases early and providing alternative management pathways for referral to doctors who have the interest and skills to work proactively within compensation systems. Such a model would be consistent with usual medical referral models, maintaining the patient’s right to choice of treating doctor.
Is Legislative Support Needed to Implement a Complex Case Management Model?
The most important aspect of implementing an effective Complex Case Management Model will be consultation and agreement between the various stakeholders, particularly the insurers who administer claims and provide funding and the doctors that provide and co-ordinate treatment.
The agreed principles do need to have a legal basis either through legislative amendment or adoption of a legally enforceable ‘Code of Practice’ that defines:
- The various relevant management roles for doctors and insurers
- Important review and decision points in case management
- Alternative management pathways
In cases where there is dispute and disagreement, which is not uncommon in a compensation setting, agreed best practice needs to be supported by the legal system to ensure that all stakeholders abide by the rules.
How Would Complex Case Management Work in Practice?
A possible approach to the medical management of injured workers has been developed by the AMA in Tasmania. There are defined alternative pathways, including a pathway for ‘Complex Cases’ where the worker’s general practitioner (perhaps supported by information from the insurer or employer) makes an assessment of prognosis early on in the course of a claim. Poor prognosis cases can be streamed into an alternate management pathway on referral by the general practitioner to another doctor with recognised skills as a ‘Complex Medical Case Manager’ (CMCM).
The role of a CMCM is to act as a trusted guide within the system with primary responsibility for the best health and rehabilitation outcome for the patient, translating sometimes conflicting messages into a coherent and understandable one to save the worker from the confusion and distress associated with uncertainty and allow focus on recovery and rehabilitation.
Most CMCM’s will be general practitioners who have an interest in working within compensation systems and have demonstrated an understanding of the role and the capacity to work to undertake this type of work. Medical specialists could also take on this role in some circumstances, particularly occupational or rehabilitation physicians.
While a Workplace Rehabilitation Provider (WRP) can assist this process in many cases, there is greater value from a trusting doctor/patient relationship in complex cases where there is potential for confusion about the primary role of a WRP. A knowledgeable and experienced doctor is best placed to achieve the best outcome in complex cases.
The flowchart below illustrates how the process might work and the various roles and review points involved.
An important component of the model will be a simple screening tool that can be used by the general practitioner to identify a potential poor prognosis. For example, this might involve assessment of factors that suggest that the worker will be off work or require workplace restrictions for a month or more.
Another important component of the model will be a role description for the CMCM perhaps expanding on the existing legislative definition of the role of PTMP detailed above. The role description would emphasise the proactive nature of the role in co-ordination of treatment and facilitation of rehabilitation and return to work in conjunction with the workplace rehabilitation provider.
SUMMARY
The development of the concept of Complex Case Management with definition of related roles and alternative management pathways has the potential to address some of the barriers to recovery for injury by simplifying interactions between injured workers and compensation systems while providing a mechanism to address concerns about doctors withdrawing their services from these systems.
Peter Sharman 04 February 2016
Statement of Roles and Interests by Author