Media Release
On Friday 09 February 2018 WorkCover Board Chair, Kathrine Morgan-Wicks confirmed the make-up of the smaller, new skills-based board in accordance with the amended Worker’s Rehabilitation and Compensation Act.
See link to Media Release below:
Media Release – WorkCover Board appointments – February 2018
Legislative Council Amendments
The originally proposed legislation relating to the makeup of the WorkCover Board was amended in the Legislative Council in late 2017.
The Draft Second Reading Speech delivered by Minister Guy Barnett stated:
“Madam Speaker, the form and function of the WorkCover Tasmania Board will be refined and provisions which have proved particularly onerous or unnecessarily complex will be amended. The membership and voting structure of the Board will be redesigned to ensure all members are equipped with the necessary skills and experience to advise and make decisions.”
The bill fact sheet relating to the Government’s proposed legislation stated:
“Amend the membership and voting structure of the WorkCover Tasmania Board to ensure the Board is equipped with the necessary skills and experience to provide advice and make decisions on the broad range of matters within its scope.”
The Clause Notes to the original amendment legislation clarified some detail:
“After commencement of the Act, the Board will comprise of two Departmental staff (including the Secretary) and five persons appointed by the Minister.”
The draft legislation stated that the Minister was to appoint 5 members to the board without any detail about the skills necessary, apart from the assumed reference to the functions of the board.
There were concerns expressed about the amendment bill as it related to the makeup of the WorkCover Board. There were jointly-expressed concerns from TCCI and Unions Tasmania about loss of employer and union representation, but otherwise the change to a “skills-based” board and the extension of voting rights to all board members received broad support. Concerns were expressed however about the absence of detail in the legislation about the type of expertise required on the board and provisions related to board positions. There was no detail in the original amendments that passed the House of Assembly about the necessary expertise of the five persons to be appointed by the Minister.
The changes, if enacted, might have led to a future minister appointing a board with a narrow set of skills, to the detriment of an effective workers’ compensation scheme for Tasmania and reduced ability to meet challenges faced in the future. It was pointed out that a broad set of skills, particularly in relation to evidence-based management of work disability and data analysis, was necessary to meet those challenges.
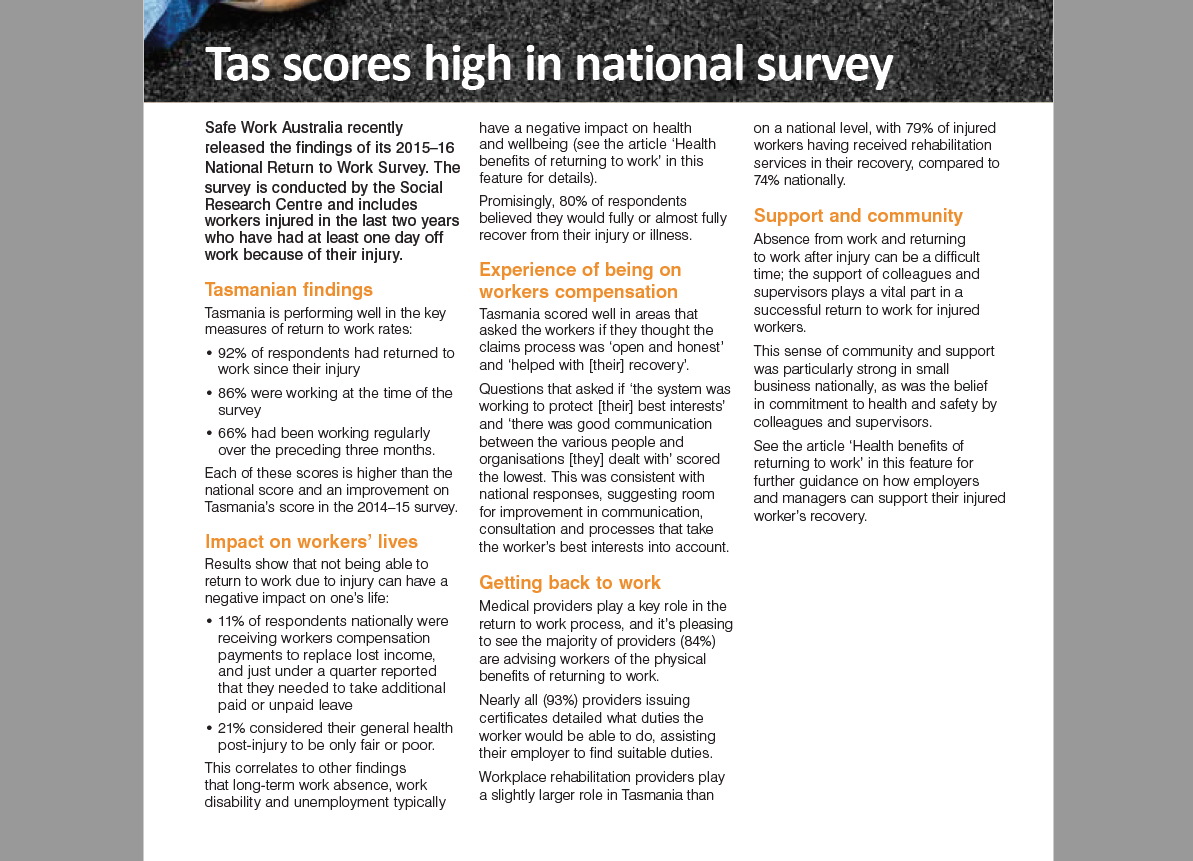
While noting positive board initiatives such as the Worker Assist service and the Better Work Tasmania initiative, I had expressed concerns including:
- There seemed to be an acceptance of rising disputation rates. (Initial disputes up from under 5% of claims in 2011/12 to nearly 8.5% in 2015/16). No measures had been introduced to improve usage of Medical Panels or other strategies to reduce disputation.
- There seemed to be an acceptance of escalating scheme legal and investigation costs (nearly $15M in the 2015-16 year and rising) i.e. significant costs to employers and the community.
- Only 45% of premium collected went to benefit injured workers. There was no data on this performance measure included in the 2015/16 Board Report.
- Concerns about the data relied upon by the board relating to Scheme Performance (Reliance on the RTW Survey and data provided by insurers)
- The Medical Mentoring Scheme (MAMS), set up to assist general medical practitioners to manage cases within the Compensation Scheme, had been abandoned.
- There has been delays in implementation of rehabilitation and medical involvement into Board processes via the Rehabilitation & Compensation Committee (although an initial meeting of the Medical Advisory Committee did occur later in 2017).
I was personally involved in presenting a submission to the Legislative Council, along with other representative health professional groups. See link below to discussion paper and briefing notes provided to the Legislative Council:
Discussion Paper for Legislative Council – July 2017
Combined Legislative Council Briefing – August 2017
Hansard (23 August 2017) provides some insight into the Legislative Council debate about this issue:
“RUTH FORREST
I am going to refer to another amendment that has been circulated, but it is not on the Table as such at the moment. I had some discussions with Dr Peter Sharman, which is probably reflected in his email to members. This is a little along the model used in Western Australia where the representative body is not prescribed, as would be in the case of the member for Rumney’s amendment, but there is a person who has expertise in work-related injuries and who advocates for, or who has experience in respect of, the interests of injured workers.
Clearly, the most well-skilled and experienced people in that area are most likely to be union officials and people who work in the union environment. They undertake those roles. It is quite likely that someone involved with the union, either in a senior way or not, could be one of the most appropriate people.
Do you name up the union and TCCI as the main representative bodies? You could argue that yes, you should, because they are the bodies that clearly represent their interests. Not everyone is a member of TCCI and not everyone is a member of a union. With medical practitioners you could say, ‘Why don’t we use a representative group there?’ Which one? The college of GPs, the AMA? Who? It becomes difficult. Lawyers – do we name up the Law Society, the Australian Lawyers Alliance? Which body?
It is difficult. If we are looking at a skills-based board, provided the skill set is identified – and this is where I think the Government was wrong in moving right away from identifying the skill set and giving all power to the minister. With all due respect to the minister; it does not matter which minister it is -“
A later amendment put forward by Ms Forrest read as follows in relation to the Board membership:
“(i) one of whom is to be a medical practitioner, or a registered nurse, with expertise in evidence-based management of work-related injuries; and
(ii) one of whom is to be an Australian lawyer with experience in workers rehabilitation and compensation matters; and
(iii) one of whom is to be a person with extensive experience in the workers compensation insurance industry; and
(iv) one of whom is to be a person with expertise in the evidence base related to management of work-related injuries and who advocates for, or has experience in respect of, the interests of injured workers; and
(v) one of whom is to be a person with expertise in the evidence base related to management of work-related injuries and who advocates for, or has experience in respect of, the interests of employers.”
This amendment was supported by the Legislative Council and later accepted by the House of Assembly.
The Legislative Council Amendments also included provision for a review of how the new board was functioning. Hansard (23 August 2017) records:
“Ms FORREST – Madam Deputy Chair, I am inclined to support that this new clause A be read a second time, because we are talking about a separate process done by an independent body. It is not just a review within the department looking at the functions of the WorkCover board. This is looking specifically at how things are functioning with this new board structure. I took on board the comments. It was a close vote on whether the member for Rumney’s amendment would be agreed to or not. If the operation of the board does not adequately see employers’ interests or employees’ interests addressed, for example, then noting that in the annual report is unlikely to occur easily. It is not going to be easily identified that is happening because it is not something the annual report is going to cover.
Sure, the annual report covers the functions of the WorkCover board and WorkSafe. I believe I have noted that report in the past, particularly when we note the workplace injuries. I was trying particularly to make the point some years ago that mining is not the most unsafe environment to work in as a lot of people think. The most unsafe environments to work in are actually the service industries, construction and forestry.
We note these reports but it does not go to the level of detail about how the board is functioning in its new format. It is reasonable that there is an independent review of this as the new clause says the independent review is to be carried out by persons who, in the minister’s opinion, are properly qualified, but also one or more who are not employees of the state or the agency of the state, so there is that independent oversight. You can confidently get input from employers and employees to be sure that everyone’s interests are being met. A friend of mine often raises concerns with me about matters that arise, such as levels of incapacity and how those things are assessed. There are opportunities to raise those things. We can ask questions and we can note an annual report, but this is not the same as the reporting them in annual reports. It is a separate process to see how the new board function is working.
If interests of the key people are not being well served, those in whose interest this bill is all about – the employers and the employees – perhaps it does need review and change. That is the only way to be really sure. An independent review would delve right into that and look at it, rather than the overarching question of how this whole department and section is working.”
The New Board
I should explain that I was an applicant for a position on the new skills-based board, but although I had an interview, I was not successful in gaining a position on the board. While there is some disappointment for me personally, there are many positives with the new board appointments and I congratulate the Government on agreeing to the legislative amendments to encourage a better set of skills on the board and the balance inherent in the new board appointees. The new board gives me hope that some of the issues with Tasmania’s workers compensation scheme can be addressed.
The appointee with expertise in the interests of employers (Julieann Buchanan) is an Occupational Therapist (OT) with significant expertise in rehabilitation and injury management, which means, for the first time, there will be expertise on the board related to this field.
The appointee with expertise in the interests of workers (Jessica Munday) has enthusiasm and understanding of the issues as they affect injured workers and experience with the Worker Assist service.
I understand the legal appointee, Mr Graham Wood has experience in acting for both insurers and injured workers.
In addition, the WorkCover Director of Compensation and Communication has changed. Vicki Tabor is an experienced health practitioner with qualifications as a registered nurse with post graduate qualifications in OHSM and Ergonomics who has worked extensively in the field of OH&S and workplace rehabilitation and, no doubt, will bring additional skills into the WorkCover organisation itself, to complement those of the board. Prior to taking on this role she was Compliance Manager with WorkSafe Tasmania.
One disappointment was that meetings of the newly formed Medical Advisory Committee/Panel to the board (consisting of John Saul [AMA]; Ian Almond [RACGP] and myself [AFOEM] has been put on hold, pending clarification as to whether the new board supports the need for this advisory group. I hope that this represents only a temporary hold on this important mechanism for medical input into the operation of the scheme.
Overall, I feel quite positive that the new board, with new and enhanced skills relating to data analysis, rehabilitation and injury management that can initiate evidence-based changes to Tasmania’s WC Scheme.
Let’s hope the legislated independent review in a few years’ time provides a positive analysis of the new board structure.
See our new republishing guidelines if you wish to disseminate this article.